It was 40 years ago that I first learned of the power of magnesium. That was during my medical training when a pulmonary specialist told us fledgling doctors that it was vital to check magnesium levels in critically ill intubated patients. The reason: suboptimal magnesium makes it harder to “wean” patients off ventilators. Even then it was known that magnesium deficiency could compromise respiratory muscles that enable patients to breath on their own.
It’s estimated that, short of overt magnesium deficiency diagnosable by a standard blood test, 60-80% of Americans have suboptimal magnesium. The consequences could be dire, since magnesium is ubiquitous in metabolic pathways that affect virtually all organ systems.
The main reasons for magnesium deficiency are 1) inadequate intake due to overconsumption of ultra-processed foods 2) medications that deplete magnesium, including acid-blockers and diuretics 3) stress, and 4) medical conditions like diabetes and ulcerative colitis that deplete magnesium.
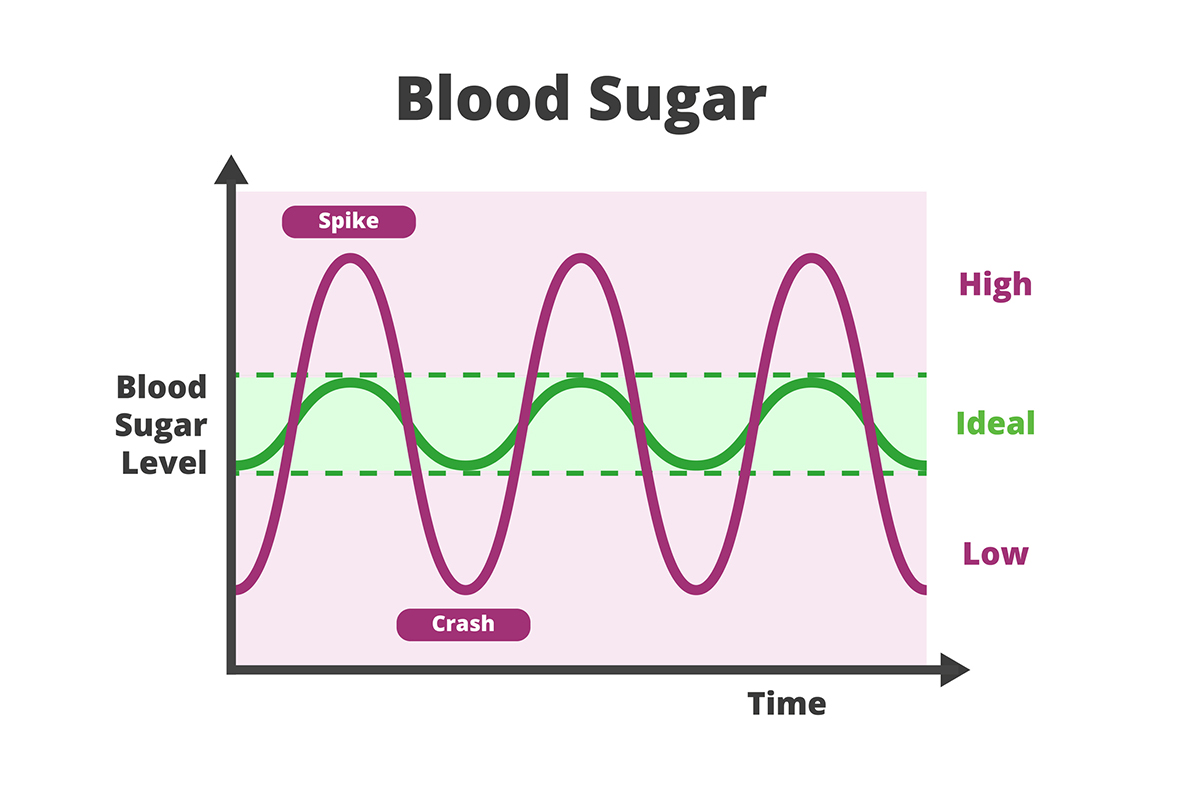
It’s an encouraging sign that the FDA—long stingy about acknowledging the benefits of vitamins and minerals—just announced authorization of a “qualified health claim” for magnesium: “Some scientific evidence suggests that diets with adequate magnesium may reduce the risk of high blood pressure.”
That’s weak tea in view of the overwhelming evidence that magnesium is essential for coronary artery disease prevention. In 2020, a huge study concluded that low magnesium was a significant risk to the heart.
Now comes evidence that magnesium impacts the immune system, too. A Swiss study just out this year demonstrates that magnesium is essential for proper functioning of T cells, the immune system’s bulwark against pathogens and cancer.
Indeed, it’s been proposed that magnesium may be important in Covid: “Magnesium deficient animals and humans have depressed immune responses, which, when supplemented with magnesium, a partial or near full reversal of the immunodeficiency occurs . . . A recent study from Singapore highlights the potential role of magnesium for improving coronavirus (COVID) outcomes.”
And lately, it’s been demonstrated that magnesium plays a crucial role in cognition. The Women’s Health Initiative Memory Study found that the greater the intake of magnesium, the lower the risk of dementia.
Magnesium’s benefits derive, in part, from its ability to activate vitamin D. “Magnesium deficiency shuts down the vitamin D synthesis and metabolism pathway,” according to a recent study.
Part of the problem is medicine’s obliviousness to the importance of magnesium. And the use of standard blood tests, which vastly underestimate magnesium insufficiency, compounds the damage.
A recent review of the subject of magnesium testing reveals, “The current ‘normal’ range interval of serum magnesium is 0.7–1 mmol/L and was established based on serum magnesium levels gathered by a U.S. study between 1971 and 1974 of presumably healthy individuals aged 1–74 years.” But what constitutes “healthy”?
Another review concludes “The perception that ‘normal’ serum magnesium excludes deficiency is common among clinicians. This perception is probably enforced by the common laboratory practice of highlighting only abnormal results. A health warning is therefore warranted regarding potential misuse of ‘normal’ serum magnesium because restoration of magnesium stores in deficient patients is simple, tolerable, inexpensive and can be clinically beneficial.”
Yet another echoes the call for more stringent standards for magnesium: “The traditional method to establish a reference interval for the serum magnesium is flawed by the large number of ‘normal’ individuals who have a subtle chronic negative magnesium balance due to a significant decrease in magnesium intake over the past century.”
Then there are the drugs. Tens of millions of Americans take powerful acid-blockers like Protonix, Prevacid, Prilosec, Dexilant, Aciphex, and Nexium. These proton pump inhibitors are now required to carry a black box warning—often ignored—indicating they can cause magnesium deficiency. Supplements may help, but a review reveals that “of 25% of cases reported to and reviewed by the FDA, magnesium supplementation alone was insufficient for correcting hypomagnesemia, and PPI therapy had to be discontinued.”
So, too, do commonly used diuretics for high blood pressure, edema, and congestive heart failure. This is especially concerning for patients at risk of heart problems. Patients taking these medications are rarely screened for magnesium levels.
I fell victim to magnesium illiteracy when I fractured my hip in a bike accident back in 2006. I was brought to the hospital by ambulance and placed on a morphine drip. I told the young orthopedic resident who admitted me—he looked about 20—that I was a doctor. I requested that I be given some magnesium via the IV catheter in my arm. He looked at me and asked why? I told him that trauma victims are notoriously prone to low magnesium—it’s a consequence of shock.
Evincing surprise, he informed me that he didn’t routinely write orders for magnesium for trauma patients, and studiously asked me if there was any peer-reviewed literature that supported my contention. I was hardly in a position to quote chapter and verse, but promised that if he would swing by my room during my hospital stay, I’d give it to him. He did, however, humor me by ordering a magnesium blood test.
I had little hope that the test would confirm my suspicions, given how insensitive it was. So I resigned myself to not getting any magnesium, although I had a friend bring me some oral supplements.
Two days later, as I lay there heavily sedated, a nurse came in and started fiddling with my IV bottles. Drowsily, I asked her what she was putting in my line. “Oh, that’s the magnesium. It says here you tested low.”
All the more remarkable, because using the standard, insensitive magnesium test, I’d never encountered a patient who walked into my office under their own power with a magnesium below the defective threshold entrenched in 1971!
It’s only in debilitated hospitalized patients—like me at the time—that low serum magnesium shows up by these unrealistic criteria.
The young orthopedic resident never did follow up to get a reference to that magnesium study. I was too debilitated to bother to track him down.
BTW, here’s a landmark article on the subject, which states: “Hypomagnesemia was the most common laboratory abnormality identified in the cohort of mildly injured victims of mostly blunt trauma.” 43% had it.
Various forms of magnesium are available: Magnesium oxide is cheap, but poorly absorbed; so is magnesium citrate, but it’s helpful for constipation and prevents kidney stones; magnesium glycinate is gentle on the stomach and supports sleep and relaxation; magnesium taurate has anti-arrhythmic and anti-seizure effects; magnesium aspartate is said to promote energy; magnesium malate is reputed to help fibromyalgia; and magnesium threonate crosses the blood-brain barrier to alleviate anxiety and improve cognition.
Foods with high levels of magnesium include dark leafy greens, beans, whole grains, dark chocolate, fatty fish such as salmon, nuts, and avocados.
(Bear in mind, this article merely scratches the surface of the myriad benefits of magnesium.)